
While standard Colorectal cancer screening initiates the oncology timeline, confirming a complex Bowel cancer diagnosis demands precise molecular staging.
Undergoing an advanced PET Scan in Bangalore allows oncologists to bypass structural limitations. By utilizing a specialized PET scan for colorectal cancer, medical teams track cellular metabolic activity in real time. The core PET CT scan benefits lie in identifying hidden metastases before surgery.
Understanding your upcoming PET scan procedure empowers you to face treatment confidently, transforming an anxious diagnostic process into a clear, actionable roadmap for recovery.
In the realm of gastrointestinal oncology, timing and structural precision dictate the success of therapeutic interventions. Standard colonoscopies and conventional imaging methods are excellent for finding primary tumors within the bowel wall.
However, they cannot always reveal the full biological picture once the disease has begun to interact with the lymphatic system or distant organs. This is where high-resolution molecular imaging becomes an absolute clinical necessity, preventing unnecessary surgical procedures and ensuring your treatment is targeted with flawless accuracy.
We believe that informed patients make the most resilient recoveries. Let us walk you through the precise science of molecular imaging, the specific scenarios where it is mandated, and how it directly shapes your path to remission.
Medical Disclaimer
The clinical insights, diagnostic protocols, and oncological staging information presented in this article are intended strictly for educational and informational purposes. This content does not constitute professional medical advice, a definitive clinical diagnosis, or a personalized surgical or therapeutic plan. Colorectal cancer presentation, metastatic pathways, and treatment regimens vary drastically from patient to patient. Always consult directly with your primary care physician, gastroenterologist, or board-certified oncologist regarding your specific symptoms, screening schedule, and diagnostic imaging needs. Never disregard professional clinical guidance or delay seeking necessary medical treatment based on the information read in this guide.
When is a PET Scan Actually Used?
When patients are first introduced to the complexities of gastrointestinal oncology, there is often significant confusion regarding which imaging test performs which function. A common misconception is that a PET scan is used as an initial screening tool to find bowel cancer. In modern clinical practice, this is not the case.
To navigate your diagnosis confidently, it is crucial to understand the distinct difference between screening (detecting the initial presence of a disease) and staging (mapping the exact extent and metabolic aggressiveness of the disease).
The Diagnostic Hierarchy
The journey from initial symptom detection to surgical planning follows a rigorous, stepped protocol. Here is how your medical team utilizes different diagnostic tools to build a complete biological profile of your condition:
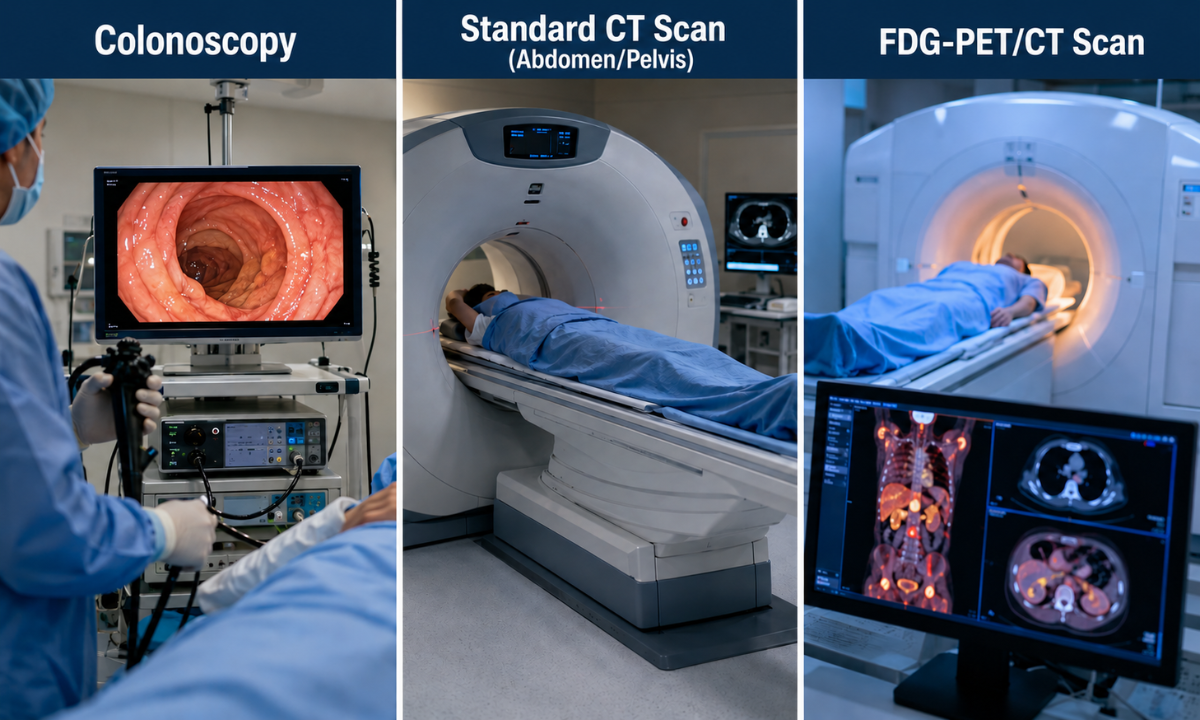
| The Diagnostic Tool | Its Primary Clinical Purpose | What It Cannot Do |
|---|---|---|
| Colonoscopy | The Gold Standard for Screening: Used to visually inspect the inner lining of the colon, locate the primary tumor, and extract tissue for a definitive biopsy. | It cannot see beyond the intestinal wall to tell if the cancer has breached the lymphatic system or distant organs. |
| Standard CT Scan (Abdomen/Pelvis) | The Anatomical Map: Used immediately after diagnosis to measure the physical size of the tumor and check for obvious structural changes in nearby organs. | It struggles to differentiate between benign scar tissue and active cancer cells, and often misses microscopic spread. |
| FDG-PET/CT Scan | The Ultimate Staging Authority: Ordered by oncologists to track the metabolic activity of the cells. It acts as a full-body radar to detect hidden micro-metastases. | It is not used for initial screening or removing polyps; its power lies in mapping the disease after initial detection. |
The Clinical Perspective: We do not use molecular imaging to simply confirm what we already know. We use it to uncover what standard imaging might be missing. If a colonoscopy confirms the presence of a tumor, a PET/CT scan answers the most critical question in oncology: “Has it spread, and exactly where is it active?”
Reserving advanced molecular imaging for the staging phase, oncologists ensure that the data collected directly influences the most critical decisions, specifically, whether a patient requires immediate surgery, targeted chemotherapy, or a combination of both.
How FDG Targets GI Tumors

To understand why a PET scan is such a powerful tool in colorectal oncology, it helps to understand the fundamental difference between anatomical and molecular imaging.
While a standard CT scan shows your medical team the physical shape and size of your internal organs, a PET scan goes a step further it reveals exactly how the cells within those organs are behaving in real time.
As specialists in nuclear medicine, we leverage a specific biological flaw within cancer cells to map the disease with pinpoint accuracy.
Exploiting the Warburg Effect
Colorectal cancer cells share a critical biological vulnerability: they are exceptionally greedy for energy.
As malignant cells are constantly dividing and multiplying at an unnatural, accelerated rate, they require massive amounts of glucose (blood sugar) to fuel their rapid growth. In clinical oncology, this intense metabolic demand is known as the Warburg Effect.
We exploit this hyperactive metabolism using a specialized diagnostic radiotracer called Fluorodeoxyglucose (FDG). Simply put, FDG is a synthetic glucose molecule that has been tagged with a microscopic, harmless radioactive isotope.
The Cellular Mechanism
Here is exactly what happens inside your body during the resting phase of your scan procedure:
- The Introduction: The FDG tracer is administered into your bloodstream via a small intravenous (IV) line in your arm.
- Cellular Absorption: Over the next 45 to 60 minutes, the tracer circulates throughout your body. The hungry colorectal tumor cells aggressively absorb the FDG, mistaking it for normal metabolic fuel.
- The Cellular Trap: Here is where science takes over. Unlike regular sugar, cancer cells cannot fully metabolize or break down the FDG molecule. Consequently, the radioactive tracer becomes securely trapped and accumulates in high concentrations strictly within the malignant cells.
- The Detection: As you pass through the advanced ring of our GE-DISCOVERY IQ GEN 2 scanner, highly sensitive detectors capture the minute energy emissions coming from the trapped tracer.
Illuminating the Disease
The scanner’s advanced software translates these energetic emissions into a high-resolution, 3D color-coded map of your body. On your oncologist’s monitor, normal, healthy tissue appears visually quiet or cool. In stark contrast, any active colorectal cancer cells light up brilliantly on the screen.
This creates an unmistakable metabolic beacon, allowing the radiologist to definitively pinpoint the primary tumor and spot any microscopic clusters of cancer cells that may have traveled to other parts of the body.
The Two Critical Scenarios for Liver Metastasis and Rising CEA
While a PET scan for colorectal cancer is an incredibly versatile tool, oncologists rely on it most heavily to navigate two specific, highly complex clinical scenarios. In both cases, standard anatomical imaging simply lacks the microscopic sensitivity required to make a definitive medical decision.
If your physician has ordered an advanced scan, you likely fall into one of these two critical categories:
Scenario A: Mapping Hepatic (Liver) Metastases

The biological reality of bowel cancer is that its venous drainage system leads directly to the liver. Consequently, the liver is the most common site for colorectal cancer cells to spread (metastasize).
When evaluating the liver, standard CT scans can easily detect large tumors, but they often struggle to distinguish small, sub-centimeter metastases from benign cysts or blood vessel clusters (hemangiomas).
Here is why a PET/CT is structurally superior for hepatic evaluation:
- The Contrast Advantage: Healthy liver tissue absorbs very little of the FDG radiotracer. This creates a visually dark background. If a microscopic cluster of hyperactive colorectal cancer cells is present in the liver, it absorbs the tracer aggressively and shines brilliantly against the dark background, making it impossible to miss.
- Surgical Impact: Accurate hepatic mapping is essential. If the scan reveals a single, isolated metastasis in the liver, your surgeon may perform a metastasectomy, a curative surgery to remove that specific lesion.
However, if the scan reveals dozens of micro-metastases scattered throughout the liver (which a standard CT might have missed), surgery is canceled, saving you from an invasive, futile procedure, and you are immediately transitioned to targeted chemotherapy.
Scenario B: Investigating a Rising CEA Blood Marker

After you have completed your initial treatment (surgery or chemotherapy), your oncologist will place you on a surveillance program. A core component of this surveillance is regular blood tests to check your Carcinoembryonic Antigen (CEA) levels. CEA is a specific protein produced by colorectal cancer cells.
When a patient’s CEA levels begin to steadily rise after treatment, it is a glaring red flag indicating that the cancer has likely recurred. However, a blood test only tells the doctor that the cancer is back; it does not tell them where it is hiding.
The Clinical Gap: In up to 30% of cases where a patient has a rising CEA level, standard CT scans and colonoscopies show absolutely nothing. The recurrent tumor is simply too small to alter the anatomical structure of the tissue.
The PET/CT Solution: When conventional imaging fails, molecular imaging takes over. Recent oncological studies demonstrated that advanced FDG-PET/CT scans possess an outstanding sensitivity of over 94% in detecting recurrent colorectal cancer in patients with rising CEA levels.
As the scanner detects metabolic hyperactivity rather than just physical size, it acts as a full-body radar, sweeping the entire lymphatic system, lungs, and pelvic cavity to find the exact cellular cluster responsible for the rising blood marker.
Pinpointing the exact coordinates of a cancer recurrence allows your medical team to immediately intervene with localized radiation or targeted surgery long before the tumor grows large enough to cause physical symptoms.
Distinguishing Scar Tissue from Active Recurrence
One of the most complex challenges in colorectal oncology occurs not during the initial diagnosis, but in the years following a successful treatment.
Colorectal cancer treatments, particularly radical pelvic surgeries and targeted radiation therapy, are highly traumatic to the local tissues.
As the body heals from these intense therapies, it naturally forms thick, dense layers of fibrotic scar tissue within the pelvic cavity and around the rectal stump. This presents a massive diagnostic hurdle for standard imaging, but it is an area where a PET/CT scan proves its absolute clinical superiority.
Mass vs. Malignancy
During a routine follow-up, a standard CT or MRI scan might reveal a new, suspicious soft tissue mass in the presacral area (the space between the rectum and the lower spine). As conventional scans rely entirely on structural size and density, the radiologist faces a critical dilemma:
Is this mass simply harmless, dense scar tissue left over from surgery, or is it a locally recurrent tumor aggressively growing back?
Standard anatomical scans cannot definitively answer this question because, structurally, a fibrotic scar and a recurrent tumor look practically identical. Before the advent of advanced molecular imaging, patients often had to undergo highly invasive, painful, and sometimes repeated biopsies just to find out.
Metabolic Tie-Breaker
A high-resolution PET scan eliminates this dangerous ambiguity by ignoring the physical shape of the mass and focusing entirely on its metabolic heartbeat.
As scar tissue is essentially dead or metabolically inactive, it does not require cellular energy. Recurrent cancer, however, is fiercely active and requires massive amounts of glucose. When the radiotracer is introduced, the difference on the scanner’s monitor is immediate and definitive:
| The Pelvic Mass | The Biological Behavior | The PET/CT Visual Result | The Clinical Action |
|---|---|---|---|
| Benign Fibrotic Scar Tissue | Metabolically inactive. Cells are not dividing or consuming energy. | Visually Cold/Dark: The mass absorbs none of the FDG tracer. | The patient is reassured. No biopsy or surgery is required. Surveillance continues. |
| Locally Recurrent Tumor | Hypermetabolic. Malignant cells are rapidly multiplying and consuming glucose. | Brilliantly Illuminated: The mass fiercely absorbs the FDG tracer, glowing intensely on the scan. | Immediate oncological intervention. The surgeon has the exact coordinates for targeted resection. |
Studies show that pelvic recurrences happen in up to 30% of operated colorectal cancer cases. By instantly differentiating between benign fibrosis and active malignancy, a PET/CT scan prevents severe surgical anxiety for healthy patients, while ensuring that those with an actual recurrence receive immediate, life-saving intervention.
Why Choose Kiran PET CT for Oncological Imaging?
When facing a complex gastrointestinal diagnosis, the margin for error is essentially zero. The quality, resolution, and expert interpretation of your molecular imaging directly dictate whether you receive the correct surgical intervention or the most effective targeted therapy.
Kiran PET CT has established itself as the Best PET Scan Centre in Bangalore precisely because we refuse to compromise on either technological capability or clinical expertise.
Oncologists and surgeons across the region consistently refer their most complex colorectal cases to our facilities in Banashankari and Indiranagar for three vital reasons:
- Next-Generation Scanning Technology: We utilize the advanced GE-DISCOVERY IQ GEN 2 imaging system. This world-class scanner provides unmatched spatial resolution, allowing our specialists to detect microscopic, sub-centimeter cellular activity in the liver and pelvic cavity that standard scanners frequently miss. Furthermore, it achieves this high-fidelity mapping while exposing the patient to significantly lower radiation doses.
- Pioneering Nuclear Medicine Leadership: An advanced scanner is only as effective as the physician reading the data. Our diagnostic team is led by globally trained experts, including Dr Kiran Kumar JK (Alumnus of PGIMER) and Dr Manoj Devanathan (Alumnus of JIPMER). Their specialized expertise in molecular oncology ensures that complex findings, such as differentiating between post-surgical pelvic fibrosis and active tumor recurrence, are interpreted with absolute clinical certainty.
In the field of oncology, anxiety thrives in the waiting room. We recognize that delayed results delay life-saving treatments. To empower your medical team to act swiftly, we guarantee that your comprehensive, cross-referenced scan reports are processed, finalized, and delivered on the very same day.
Conclusion
Navigating a colorectal cancer diagnosis is undeniably daunting, but the advent of advanced molecular imaging has radically changed how the disease is managed. A PET/CT scan removes the clinical guesswork from the equation. By mapping the exact metabolic footprint of the cancer, it prevents patients from undergoing unnecessary, futile surgeries and ensures that every single therapeutic intervention is targeted with microscopic accuracy.
When your medical team is armed with clear, definitive molecular data, your treatment plan transitions from a generalized approach to a highly personalized, confident roadmap for recovery. We are dedicated to providing the exact clarity you need to move forward with certainty and reclaim your health.





