Thyroid cancer (TC) is the most common endocrine malignancy and the ninth most common cancer in the world, based on 2020 data. It mainly affects women, with a female-to-male ratio of 3:1. Most cases of thyroid cancers originate from follicular cells, and well over 95% of all thyroid carcinomas are differentiated thyroid carcinomas (DTCs). DTC encompasses papillary thyroid carcinoma (PTC) at 85% and follicular thyroid carcinoma (FTC) at 2–5%. The other less common but more aggressive forms include poorly differentiated thyroid carcinoma (PDTC) at 1–3% and anaplastic thyroid carcinoma (ATC) at 1–3%.
Standard management of DTC patients involves total thyroidectomy combined with radioiodine (I-131) therapy (RAI). Treatment response is evaluated by measuring biochemical markers, such as thyroglobulin (Tg) and thyroglobulin antibody (Tg-Ab). Poorly differentiated and anaplastic thyroid cancers often lose the iodine uptake function, and they are thus categorized as radioiodine-refractory DTCs. The detection and management of these types of tumors are difficult. Fluorodeoxyglucose positron emission tomography/computed tomography ([18F]FDG PET/CT) has been one of the important imaging modalities in the diagnosis of recurrence and metastasis in radioiodine-resistant thyroid cancer; however, its sensitivity is 68.8-82%. Thus, there is always room for better sensitivity diagnostic tools. FAPI PET/CT is the latest window for thyroid cancer imaging and appears to be a game-changer when FDG PET/CT cannot provide adequate information.
This article will describe the role of FAPI PET/CT in the assessment of thyroid cancer, its superiority over conventional imaging methods, and its potential to change patient management.
Understanding Radioiodine-Resistant Thyroid Cancer (RAI-R TC)
Radioiodine-resistant thyroid cancer is a term used to describe DTC cases where the tumor no longer absorbs iodine, thus rendering radioiodine therapy ineffective. This condition includes:
- Negative I-131 whole-body scans (WBS) despite elevated Tg levels.
- Inability to progress in disease despite documentation of initial iodine uptake.
- Non-remission even following high cumulative doses of I-131 (>600 mCi).
- Non-avid lesions at presentation or during progression of disease.
- FDG-positive, I-131-negative lesions. This is also known as TENIS syndrome, observed in a proportion of post-treatment DTC patients up to 27%.
In these scenarios, other imaging modalities such as [18F] FDG PET/CT and FAPI PET/CT play an important role in accurate staging and treatment planning.
Limitations of [18F]FDG PET/CT in Thyroid Cancer Imaging
The American Thyroid Association suggests that in patients with RAI-refractory DTC, PET/CT [18F]FDG can be used to identify tumor recurrence and metastasis. However, it has its drawbacks:
- Incorrectly negative results in LNs: Since FDG PET/CT is dependent on the resolution, small-sized lesions may remain undetected 1–2 mm in size.
- Incomplete detection of iodine-negative lesions: Even a few large size metastatic lesions remain unnoticed.
- High glucose uptake (flip-flop phenomenon): The dedifferentiated tumors return their iodine uptake to high glucose metabolism, which makes FDG PET/CT useful but not infallible.
Taking into account the above limitations, a promising alternative for thyroid cancer imaging has emerged: FAPI PET/CT.
FAPI PET/CT: Revolution in Thyroid Cancer Imaging
The development of FAPI-based radiotracers has revolutionized the landscape of oncological imaging by targeting the fibroblast activation protein, which is overexpressed in tumor-associated fibroblasts. Some of the developed FAPI-based radiotracers include:
- [68Ga]Ga-FAPI-02, -04, -46
- DOTA.SA.FAPi
- DOTAGA.(SA.FAPi)2
These radiotracers have received much attention due to their ability to image different cancers, including thyroid cancer.
Advantages of FAPI PET/CT in Thyroid Cancer
Improved Detection of Metastases
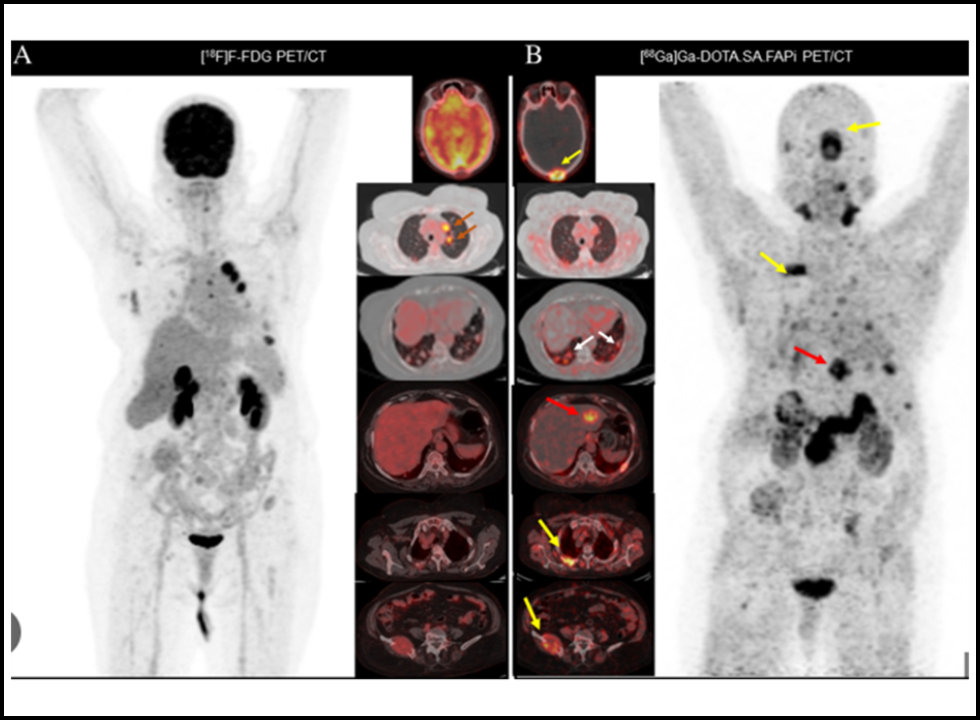
Higher sensitivity of [68Ga]Ga-FAPI PET/CT in the detection of lymph node metastases, liver metastases, brain metastases, and bowel metastases in comparison to [18F]FDG PET/CT; it has fewer false-positive and false-negative rates, especially in lung metastases.
- Better Detection of Bone Metastases
- Bone metastasis is one of the commonest places of aggressive spread of thyroid cancer and FAPI tracer is much more sensitive in comparison to FDG PET/CT.
- More sensitive in TENIS Syndrome
- More lesions are detected by [68Ga]Ga-FAPI PET/CT than by FDG PET/CT in patients with TENIS syndrome.
- Lesions are negative on FDG PET/CT but present with high FAPI uptake; thus, it can be hypothesized that FAPI PET/CT can detect non-FDG-avid lesions.
Correlation Between Tumor Size and FAPI Uptake
- Large tumor sizes display high [68Ga]FAPI uptake; this might be because of high expression of FAP in aggressive subtypes.
- Enhanced Stroma-Targeted Imaging
- Tumor lesions >1–2 mm in size require supporting stroma.
- Because stroma volume can be higher than tumor volume, FAPI PET/CT is more sensitive than glycolysis PET imaging with [18F]FDG PET/CT for non-FDG-avid lesions.
Clinical Use of FAPI PET/CT in Thyroid Cancer
Restaging of DTC
There is data indicating that [68Ga]FAPI PET/CT is more sensitive than FDG PET/CT for the detection of cervical lymph nodes and pulmonary metastases, which are the two most common metastatic sites in DTC.
Combination of FAPI PET/CT with FDG PET/CT
The two are used together to improve diagnostic accuracy. If FDG PET/CT is insufficient alone, then FAPI PET/CT completes metabolic imaging with direct tumor stroma imaging.
Theranostic Utility of FAPI PET/CT
FAPI-based radiotracers can act as theranostic agents with integrated imaging and targeted therapy. The compound [68Ga]Ga-DOTA.SA.FAPi, in particular has been found to be associated with highly selective uptake in tumors opening prospects in the precision treatment of FAPI-positive cancers.
Challenges and Considerations
Although several benefits are available, FAPI PET/CT still poses several drawbacks:
Physiological uptake of [68Ga]FAPI-04 occurs in myelofibrosis, reactive lymph nodes, arthritis, subcutaneous fibroma, thyroiditis, and follicular thyroid adenoma with fibrosis and calcification.
It may lead to a false positive in some cases and should be treated accordingly in the clinic with proper interpretation.
Conclusion
One of the most promising diagnostic modalities in thyroid cancer, FAPI PET/CT is especially useful in radioiodine-refractory cases and TENIS syndrome, thus it surpasses [18F]FDG PET/CT, with better lesion detection and increased sensitivity of imaging and theranostic potential.
Given that FAPI PET/CT can also identify lesions not seen with FDG-avid agents, bone metastases, and stroma-rich tumors, it may be an emerging new option for the imaging of thyroid cancer. Its ability to improve diagnostic accuracy of the imaging test either in isolation or in combination with FDG PET/CT would readily enhance staging and planning for treatment.
Technologies such as PET scan are likely to shift the landscape for thyroid cancer care, providing precise medicine solutions that target FAPI-positive cancers with FAPI-based imaging and therapy.





