Clinical details:
-
- A 40 year old woman presents with chief complaints of generalized fatigue, bone pain and gastritis.
- On laboratory workup – S.calcium -11.1 mg/dl, S.phosphorus – 2.7 mg/dl, and iPTH>500.
- USG neck revealed a soft tissue dense nodular lesion in close proximity to the right lobe of the thyroid gland, near its inferior pole.
- The patient was referred for a 68Ga-DOTANOC scan.
Clinical details:
Whole body PET scan was done 60 minutes after i.v. Injection of 5 mCi of 68-Ga-DOTANOC. The study was acquired using a whole-body dedicated GE DISCOVERY IQ Generation 2 PET – CT Scanner. PET images are reconstructed using advanced application Q. clear. Standard uptake values (SUV) normalized to body weight obtained over lesions.
Clinical details:
- An SSTR receptor expressing well defined peripherally enhancing soft tissue dense lesion with cystic components was noted postero-inferiorly in relation to the right lobe of the thyroid gland, measuring 2.1 x 1.9 cm – suggestive of a right inferior parathyroid adenoma.
- SSTR receptor expressing osteolytic lesions with enhancing soft tissue components are noted in multiple skeletal sites:
- Multiple sites in the skull – left occipital bone.
- Left maxilla
- Bilateral scapulae, sternum, bilateral clavicle.
- Multiple sites in bilateral ribs.
- Multiple sites in the pelvis – left iliac bone
suggestive of multifocal osteitis fibrosa cystica(Brown’s tumor)

Fig 1 : MIP images demonstrate multiple foci of increased tracer uptake, corresponding to skeletal sites.
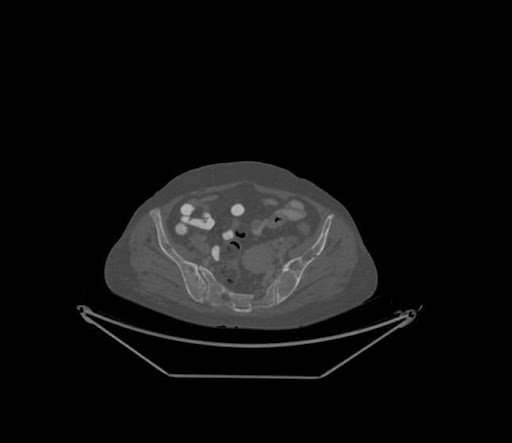
Fig 2 : CT images reveal multiple subtly enhancing soft tissue dense lesions noted in the pelvic skeleton.

Fig 3 : The aforementioned lytic lesions demonstrate intense DOTANOC avidity as illustrated above.
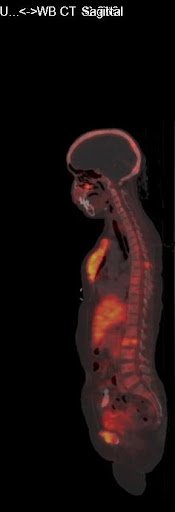
Fig 4 : Sagittal images reveal multiple other foci of tracer avid lytic lesions, most notably the sternum which demonstrates an intensely tracer avid expansile lytic lesion.

Fig 5 : CT images of the neck reveal a heterogeneously enhancing soft tissue dense nodular lesion posterior to the right lobe of the thyroid gland – likely a parathyroid adenoma.
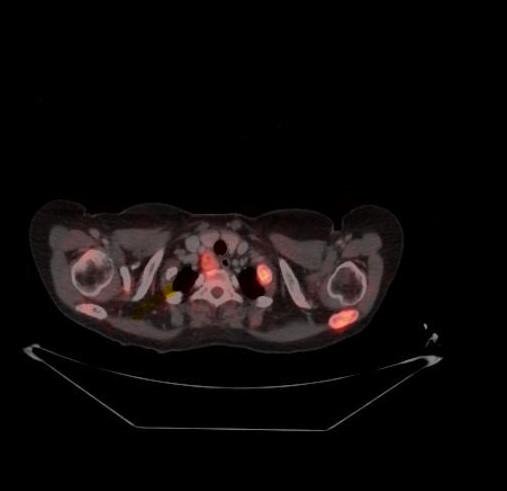
Fig 6 : The aforementioned lesion demonstrates increased DOTANOC avidity.
DISCUSSION:
- A parathyroid adenoma is a benign tumor of the parathyroid glands. The parathyroid glands are located in the neck, near or attached posterior to the thyroid gland.
- The parathyroid glands in the neck help control calcium use and removal by the body. They do this by producing parathyroid hormone, or PTH. PTH helps control calcium, phosphorus, and vitamin D levels in the blood and is important for healthy bones.
- Parathyroid adenomas are common. Most parathyroid adenomas do not have an identified cause. Sometimes a genetic problem is the cause. This is more common if the diagnosis is made when you are young
- Many people have no symptoms. The condition is often discovered when blood tests are done for another medical reason.
- Parathyroid adenomas are the most common cause of hyperparathyroidism (overactive parathyroid glands), which leads to an increased blood calcium level.
- Symptoms may include any of the following:
- Confusion
- Constipation
- Lack of energy (lethargy)
- Muscle pain
- Nausea or decreased appetite
- Urinating more often at night
- Weak bones or fractures
- Brown’s tumor – osteitis fibrosa cystica – exaggerated bone resorption resulting in fractures.
- Renal stones.
- Gastritis.
- psychosis.
- Blood tests may be done to check levels of:
- PTH
- Calcium
- Phosphorus
- Vitamin D
- A 24-hour urine test may be done to check for increased calcium in the urine.
- Other tests include:
- Bone density exam
- Kidney ultrasound or CT scan (may show kidney stones or calcification)
- Kidney x-rays (may show kidney stones)
- MRI
- Neck ultrasound
- Sestamibi neck scan (to identify the location of the parathyroid adenoma)
- Surgery is the most common treatment, and it often cures the condition. But, some people choose to only have regular checkups with their health care provider if the condition is mild.
ROLE OF GALLIUM DOTANOC PET/CT:
- Parathyroid adenomas and brown’s tumors express SSTR receptors, which has a high affinity for DOTANOC.
- Ga-68 DOTANOC scan aids in the:
-
- Diagnosis and localisation of the parathyroid adenoma.
-
- Identifying sites of brown tumour.
-
- Identifying sites which are prone to fractures and which need urgent care – i.e neck of the femur.




